by Lauren Thompson, Jennifer Reardon, Joy Howard, and Sarah M. Jackson
Share
Ancient history and literature often illuminate modern times. In Homer’s epic poem, The Odyssey, the warrior-king Odysseus leaves his wife and infant son to fight in the 10-year Trojan War. His journey home lasts another decade and tests every fiber of his being.
The resilience, luck, and help required for Odysseus’ return may resonate for anyone dealing with mental illness. In this country alone, millions of people endure decades-long odysseys through mazes of mental health obstacles, including an insurance system that can thwart seekers and providers of mental health care alike.
To better understand and document some of their heroic ordeals, we spoke with more than 40 patients, providers, and researchers in the Brigham Health community. They shared stories of trauma and healing, despair and resolve, disparity and innovation, stigma and triumph.
And they are not giving up.
David Silbersweig, MD, chair of the Brigham and Women’s Hospital Department of Psychiatry, is one of many people determined to improve care and the ways people access it—and to destigmatize mental illnesses.
“Psychiatric disorders are real medical disorders, and they are ubiquitous,” Silbersweig says. “Every year, one in four people is affected. When you add addictions, it goes way beyond that. And when you add comorbid medical illness, which most people have by the time they’re older, the rate goes way up again. Every family is affected.”
Honoring these stories has left us heartbroken and inspired, frustrated and determined. Perhaps the people you meet in the following pages will leave you feeling similarly. If you, like so many, are in the midst of this odyssey, we are with you. If this is new to you, we invite you to join us on the journey.
1
Assessing
the Challenge
Surveys consistently show that 25% of adults in developed countries experience significant mental health problems each year.
I. “We’ve all had the common cold form of mental illness”
What percentage of people would you guess have had a mental illness in their lifetimes? It depends on your definition of mental illness. What if the question were broader: What percentage of people would you guess have had any illness in their lifetimes?
“No one would be shocked if we learned that 99% of people had a physical illness during their life, whether it’s a cold or cancer; likewise, we’ve all had the common cold form of mental illness at some point,” says Ronald C. Kessler, PhD, a world-renowned expert in surveying global mental health and the McNeil Family Professor of Health Care Policy at Harvard Medical School.
Kessler continues, “For example, many people who have just broken up with a boyfriend or girlfriend will meet the criteria for major depression. Does it mean they need psychotherapy? No. Would psychotherapy help? Maybe. That’s a common cold version of mental illness. The more important question is: Who has a persistent, severe mental illness that is derailing their life?”
From 1990 to 1992, Kessler conducted the first community-based epidemiological survey of mental disorders among adults in the United States. Over the next 25 years, he replicated and extended the study throughout the world.
Kessler’s surveys have helped define the prevalence of severe mental disorders, which he describes as “looking like a bullseye.” At the center are the 2% to 4% of people clinically diagnosable with schizophrenia, bipolar disorder, severe depression, and other conditions. Moving further out, another 6% to 8% of people report other moderate to severe mental health issues that interfere with their lives. These rates of mental illness in the U.S. haven’t changed for more than 60 years, despite increasing awareness and improved treatments.
“Surveys consistently show that 25% of adults in developed countries experience significant mental health problems each year,” says Kessler. “This prevalence, coupled with the high impairment of these conditions, led the Global Burden of Disease Study to conclude that mental disorders account for more global impairment than any other class of non-communicable diseases and more than all communicable diseases combined.”
Ronald Kessler, PhD, recalls this near-unanimous response from survey participants when given a hypothetical choice.
View Transcript
We’ve done this analysis in many countries, the same kind of questions. And so we have hundreds of thousands of people we’ve interviewed, and we have enough people that we can say, well look we have 2,700 people who both have depression and have diabetes. So we say good, you know what it’s like to have diabetes, you know what’s like to have depression, or asthma. And what would you do if I had the one magic pill, which pill would you want, the one to make the diabetes go away or the one to make the depression go away? Everybody, in every country around the world, wants the pill to make the depression go away.
Repeated national surveys show nearly 60% of people with mental illness didn’t receive mental health services in the previous year. The complexity and stigma attached to these conditions have led to mental health care in the U.S. being separate and unequal from medicine for physical diseases.
“Despite widespread suffering, we are doing the equivalent of 1950s cardiology in the mental health field,” says Kessler. “We don’t have the equivalent of a statin or cholesterol pill yet. So we’re waiting for the equivalent of a heart attack—the suicides, overdoses, or violent outbursts—to occur before we do anything. Mental disorders are chronic illnesses, but our healthcare system treats them as acute, episodic illnesses. That needs to change.”
Silbersweig acknowledges the difficulties of changing the paradigms of understanding, diagnosing, and caring for people with mental illnesses.
“It’s taken longer than cardiology or other fields because we’re dealing with the most complex functions of the most complex organ that make us who we are as human beings,” says Silbersweig. “That’s also why these are among the most poignant of disorders: because they affect our individuality, relationships, identity, control of our own mind and behavior, and our subjective experience and emotions.”
II. “Even kids often can’t get the care they need”
Worldwide, half of all mental illness symptoms begin to appear by age 14 and three-quarters by age 24.1
“Anxiety disorders in children, such as phobias and separation anxiety, may not seem like a big deal when they’re just starting, but they can be a warning sign of what’s to come,” says Kessler. “Kids who are seriously depressed or anxious and who have middle-class parents might get treatment, but not very many. The United States has fewer than 10,000 child psychiatrists for 50 million kids.”
With suicide as the second leading cause of death in people between the ages of 10 and 24, untreated mental illness is a significant threat to children and adolescents, notes David Gitlin, MD, vice chair of clinical programs in the Department of Psychiatry.
“It’s unbearable to think of children dying from cancer, and so as a society we have rallied around finding cures for childhood cancers, even though most people with cancer are older,” Gitlin says. “Yet we can’t seem to get any traction about children’s mental health care. That’s how tough the stigma is. Even kids often can’t get the care they need.”
III. “I used to tough it out”
Liz* first started feeling depressed as a teenager.
“I used to tough it out,” she says. “It wasn’t until my late 20s that I tried an antidepressant after going into a much deeper depression. I didn’t know what bipolar was all about until I had a full mania a few years later.”
A decade ago, Liz received the diagnosis of Bipolar Disorder I, which causes manic and depressive episodes.
“I’ve had to practice a lot of radical acceptance with this disease,” says Liz. “I had a lot of shame when I was first diagnosed, but my therapist pointed out I wouldn’t have shame if I were diabetic or had cancer. It’s something I still struggle with.”
Several of Liz’s family members also have mental illness. Her sister has been treated for panic disorder and depression. Her father has experienced depression. And her paternal grandmother received a bipolar diagnosis late in life. As Liz responds to each flare-up of her disease, her family remains her biggest support, including her husband and her mother, a nurse.
“I couldn’t have done it without them,” Liz says. “I don’t know if I would be here today without them, honestly. It’s that hard.”
Part of managing her disease, she says, is knowing when she needs help beyond regular visits with her psychiatrist and therapist close to home in the Boston suburbs. When her suicidal thoughts would not budge earlier this year, she came to the Emergency Department (ED) at Brigham and Women’s Faulkner Hospital, part of Brigham Health.
“I had asked my outpatient psychiatrist for help,” she says. “He increased my medications, but I still thought about harming myself. It was a red flag.”
After a week in the Faulkner’s inpatient psychiatric unit, Liz transitioned to the Partial Hospitalization Program in the same building. She spent five hours a day in group therapy sessions and individual meetings for six days before completing her treatment.
“I got through the most uncomfortable feelings of anxiety and depression by using tools I learned in the program,” she says. “Whether it’s meditating or taking the time to sit and read a book or going for a walk with the dog. It’s challenging, but I’m finding ways to live with it.”
IV. Stressed emergency departments
On any given day across the country, thousands of people like Liz come to hospital EDs in search of relief from symptoms of mental illness, only to find themselves at the mercy of an overburdened mental health care system.
During the past six years, the number of patients seeking emergency mental health care at the Brigham (in EDs at the main campus and the Faulkner campus) increased from 3,500 to 4,600 per year. However, these numbers do not reflect the total number of people who come to the EDs in need of mental health care.
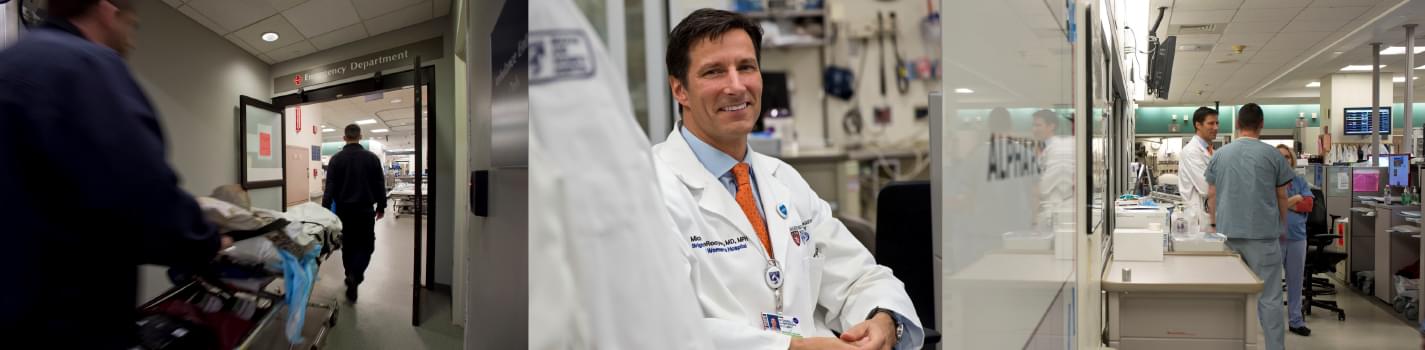
The Department of Emergency Medicine, led by Michael VanRooyen, MD, MPH (center), treats more than 4,600 patients each year for mental health emergencies. (Photo by Len Rubenstein)
“A lot of people arrive with substance use disorder, alcoholism, drug overdose, and pain issues as their main concern, who also have overlying psychiatric complaints,” says Michael VanRooyen, MD, MPH, chair of the Brigham’s Department of Emergency Medicine. “The Brigham ED is adept at managing people’s acute psychiatric complaints, particularly if they’re agitated or potentially violent. When patients require extended care, we try to move them to our inpatient psychiatric facility at the Faulkner campus, which has 24 beds.”
To better accommodate patients experiencing mental health crises, the Brigham ED is adding a Behavioral Health Care Unit as part of its expansion, expected to be completed by late 2021. The unit will provide a safe, quiet place for vulnerable patients to receive the treatment they urgently need. The staff’s goal is to resolve patients’ symptoms and discharge them or to manage their conditions before transferring them to an inpatient psychiatric facility.
V. “It’s too much”
It’s 8 a.m. on a Tuesday. Sejal Shah, MD, chief of the Brigham’s Division of Medical Psychiatry, heads to the ED for her morning rounds. She leads the hospital’s psychiatric consultation liaison service, the most consulted specialty throughout the Brigham Health system. In addition to the ED, units such as general medicine, oncology, cardiology, and OB/GYN call on consulting psychiatrists to assess patients and provide recommendations for care.
Today, Shah has two psychiatric patients to see in the ED. Often, there are as many as eight.
Ellen* lies on a gurney in a treatment bay—one of two in the ED with a retractable metal door installed in the back. Any medical equipment Ellen could use to harm herself is secured behind the door. The overhead lights are dimmed. Her Bible and her unfinished breakfast sit on the tray table next to the bed. A personal care assistant sits nearby, assigned to watch her.
Sejal Shah, MD, is a consulting psychiatrist in the ED. (Photo by Stu Rosner)
She has been here 36 hours, waiting for a bed to open up at an inpatient psychiatric facility. Shah enters and asks Ellen a series of questions, including, “Are you having any thoughts of not wanting to live anymore or wanting to hurt yourself?”
Still recovering from recent drug use and a head injury, Ellen replies, “Not right now.”
Building a 'More Humane' ED
Expanding the Brigham’s emergency department will provide safer and more private care for patients in crisis.
It’s a relatively quiet morning in the Alpha pod of the ED, where the most acutely ill or injured patients receive care. At any moment, patients can be rushed in with anything from a heart attack to a severe injury to a gunshot wound. Asked what it’s like for her in this environment, Ellen slumps and shakes her head, “It’s too much.”
This is Ellen’s second time in the Brigham’s ED in the last week. She hopes an inpatient facility can help her recover from addiction and depression so she can get back home to her 3-year-old son, who is being cared for by her mother.
Shah ends the conversation, saying they are looking for a bed for her. After 34 more hours in the tiny room, nearly three full days in total, Ellen transfers to an inpatient facility.
“The system is so broken,” says Shah. “We’re grossly under-bedded. Patients can board for days in the ED waiting for an inpatient bed. And Massachusetts is one of the better states. In other states, patients can wait for weeks or months. More often, nothing is available, so they get discharged without their needs being met.”
*All patient names have been changed to protect privacy.
2
A Broken System —
by Design
We have an attrition model of mental health care that demands people put in all this work just to find a provider and make an appointment.
VI. Provider shortages and ghost networks
People seeking outpatient psychiatric treatment can also endure long waits to get help. Gitlin points to severe shortages of mental health providers across the country. For example, nearly 80% of counties in Montana don’t have a single practicing psychiatrist.
“While things are better in Massachusetts than in many other places, it can still be difficult to find a psychiatrist,” Gitlin says. “There aren’t nearly enough available for the number of people who need them.”
In a 2015 study exploring the difficulties of finding a psychiatrist, researchers posing as patients called 360 in-network psychiatrists in Houston, Chicago, and Boston. Using phone numbers provided by a major insurer, researchers attempted to make appointments claiming to have Blue Cross Blue Shield, Medicare, or the willingness to pay out of pocket.
The results were damning. More than 15% of the phone numbers on the insurer’s lists were wrong; they included numbers for restaurants, boutiques, and jewelry stores. Still, other numbers led to providers who were dead. When callers did reach practicing psychiatrists’ offices, many doctors didn’t accept insurance or weren’t taking new patients.
After calling every number twice, researchers were unable to make appointments with 74% of providers on the insurer’s lists. For a similar study among pediatric psychiatrists, researchers were unable to make appointments with 83% of the providers listed as in-network by Blue Cross Blue Shield. Inaccurate provider lists are so common, they have a name: ghost networks.
Between provider shortages, ghost networks, and insurance coverage limits, many people have no access to affordable and effective mental health treatment, even in a crisis. According to the National Alliance on Mental Illness, an estimated 43.6 million adults in the U.S. experienced a mental health condition in 2014, but only 41% of them received mental health services.
“We have an attrition model of mental health care that demands people put in all this work just to find a provider and make an appointment,” says Gitlin. “On top of that, they often have issues with finances, transportation, work, housing, and relationships. All of these things interfere with their ability to get the treatment they need.”
VII. Discrimination “infected” by financial incentives
If you come into the ED with appendicitis…you can be admitted no matter what your insurance situation is…. But mental health is completely different.
“If you come into the ED with appendicitis or some other medical issue needing hospitalization, you’re admitted no matter what your insurance situation is, no questions asked,” says Paul Chen, MD, director of clinical operations in the Brigham’s ED. “But mental health is completely different. If we determine you are suicidal and need to be admitted to the hospital, we have to get authorization from the insurance company about whether you can be admitted. The insurance company can say no, triggering an appeals process between our psychiatry team and the insurer that can delay when patients get to a psychiatric facility or result in the patient going to a lower level of care.”
The Mental Health Parity and Addiction Equity Act of 2008 is a federal law intended to eliminate discrimination by requiring insurers to cover illnesses of the brain, such as depression or addiction, with no more restrictions than illnesses of the rest of the body, such as cancer or diabetes.
Without biological markers of mental illness, insurers can—and frequently do—deem mental health services as medically unnecessary, enabling them to deny claims outright or reduce reimbursements. But the tide may be turning.
In March 2019, a U.S. federal judge ruled that United Behavioral Health (UBH), a subsidiary of the nation’s largest health insurer, illegally denied coverage to tens of thousands of subscribers with mental health or substance use needs, many of them children. In his 106-page decision, Chief U.S. Magistrate Judge Joseph Spero says the insurer’s internal policies were “infected” by financial incentives created to restrict coverage for mental health and substance use treatment in order to cut costs.
While insurers use widely different criteria for covering mental health and addiction care, medical experts have sought to establish standard guidelines. For example, many states now require providers and carriers to use addiction-treatment criteria developed by the American Society of Addiction Medicine (ASAM). Spero specifically cites these criteria in his ruling.
“UBH’s refusal to adopt the ASAM criteria was not based on any clinical justification,” Spero writes. “Indeed, all of its clinicians recommended that the ASAM criteria be adopted. The only reason UBH declined to adopt the ASAM criteria was that its finance department wouldn’t sign off on the change.”
Spero adds, “It is well-established that effective treatment of mental health and substance use disorders includes treatment aimed at preventing relapse or deterioration of the patient’s condition and maintaining the patient’s level of functioning. UBH Guidelines deviate from that standard.”
UnitedHealthcare, the parent company of UBH, has not announced whether it will appeal Spero’s decision. In the next phase of the case, the parties involved will present arguments about appropriate remedies.
VIII. “In an ideal world, I shouldn’t have to do this job”
Sparring with health insurers over the dearth of inpatient psychiatric beds has become a complex job for Jessica Rosado, MA, LMHC, utilization manager for the Faulkner’s Department of Psychiatry. Rosado works mostly on behalf of people already admitted to the hospital’s inpatient psychiatric unit, which is designed for short-term, acute care.
Michael VanRooyen, MD, MPH, calls out the challenges facing emergency departments across the country.
View Transcript
The needs of psychiatric patients are growing. We have more of them than there are psychiatric beds that are available in the state. In some states, it's disastrous. In our state, it's still very challenging. So it has to do with the difficulty in accessing both outpatient and inpatient psychiatric services. And frankly, what happens is the EDs are boarding these patients for, you know, days.
“Our average length of stay is 10 days,” says Rosado. “But if one of our patients needs continuing care and isn’t safe to be discharged, we apply for them to go to a state psychiatric hospital.”
The catch? In recent years, the wait time for a bed at state-run psychiatric facilities has nearly doubled.
“It used to take three months for patients to get a state psychiatric bed, but now it’s more like five months,” Rosado says. “The Massachusetts Department of Mental Health is aware they don’t have enough beds for people, but we can’t speed up the system. Since we never discharge a patient for lack of insurance, some patients end up waiting here for a state bed longer than they’ll stay there. As a result, those beds are not available for the next patients who need them.”
“It used to take three months for patients to get a state psychiatric bed, but now it’s more like five months.” – Jessica Rosado, MA, LMHC
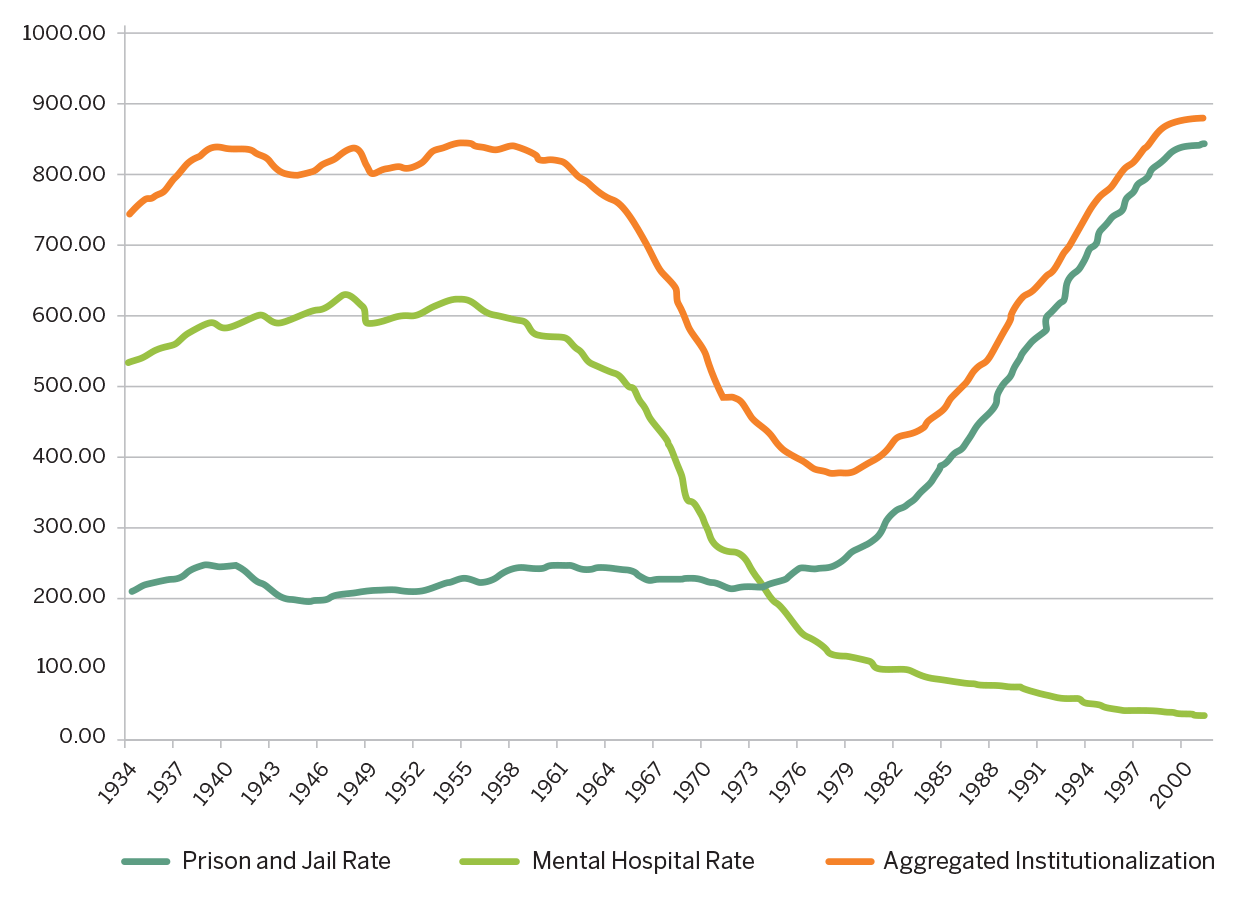
Hospitalization to Imprisonment
Since the 1950s, closures of state-run psychiatric hospitals helped fuel a new crisis: mass incarceration. READ MORE
Despite this well-known bed shortage, Rosado frequently contends with insurers that don’t want to fully cover care for patients staying at Faulkner while they await admission to a state psychiatric hospital.
“In an ideal world, I shouldn’t have to do this job,” says Rosado. “Even when we can show a patient isn’t ready to be discharged and has nowhere else to go, insurance companies often argue it’s not necessary for them to receive acute care in our inpatient psych unit. Then they pay us 10% of what our care costs.”
This cascade of backups—at state psychiatric hospitals, at hospitals with psychiatric inpatient units, and in the ED—increases costs and stresses an already overwhelmed system and the vulnerable people in it.
3
Navigating
Obstacles
People don’t no-show their virtual visits. It expands our ability to meet with people in a way that’s convenient for their schedules.
IX. “There is so much room to try new things”
With systemic forces working against patients’ access to care, mental health leaders at the Brigham are finding workarounds for their patients. In 2018, outpatient psychiatry leaders came up with a solution to skip long wait times for appointments or visits to the ED: an urgent care clinic devoted to mental health.
Led by psychiatrist David Kroll, MD, the LUCY Clinic (short for Longitudinal Urgent Care Psychiatry) at the Brigham is open to patients who have a time-sensitive need for care but are not in immediate physical danger. Kroll sees people whose prescriptions have run out but they can’t get an appointment with their regular prescriber for weeks, or who have recently moved and don’t have a local provider.
Kroll says the clinic has been a lifeline for many patients, especially those who have Medicaid. This particular population disproportionately miss scheduled psychiatry appointments due to circumstances beyond their control, such as transportation problems, inflexible work schedules, or family responsibilities. Since psychiatry practices often drop people who have no-showed, these patients frequently end up at square one.
“It continues to shock me how great the need is for this kind of program,” Kroll says. “A lot of people aren’t able to access care for reasons that should be surmountable, like setting appointments months out or enforcing no-show policies. Our clinic provides one relatively simple solution—getting rid of the scheduled appointment altogether.”
He adds, “Behavioral healthcare is an area where there is so much room to try new things and fill big gaps. And we’re encouraged to do that here at the Brigham and to take apart these barriers that have existed for a long time.”
David Kroll, MD (left), meets with a patient in the LUCY Clinic. (Photo by Jesse Costa/WBUR)
Claire Twark, MD, and other Brigham Health psychiatrists are helping patients navigate barriers to psychiatric care through a 21st century version of the house call: virtual visits, accessible through computers or mobile devices. Virtual visits are available to patients when it’s clinically appropriate—such as for busy students, stay-at-home parents, or patients who live far away from the clinic.
“People don’t no-show their virtual visits,” Twark says. “I’m meeting with them while they’re sitting in an empty classroom, in their car, in their office, or on their lunch break. It expands our ability to meet with people in a way that’s convenient for their schedules.”
X. Integrated care, better care
In a small examination room, Jordan* and his primary care physician, Gail Levine, MD, settle into their chairs.
“How has your energy level been lately?” Levine asks.
“I get pretty tired,” Jordan responds.
Jordan has anemia and extreme fatigue, side effects of the Crohn’s disease that attacks his gastrointestinal tract. His visiting nurse has been trying to schedule him for an iron infusion, but he hasn’t answered phone calls from the clinic. Levine asks him why not, and Jordan says he doesn’t pick up calls from phone numbers he doesn’t recognize. Then, he shifts in his chair. “Actually, is there a co-pay?”
David Gitlin, MD, describes how society views suffering from mental disorders differently from other physical illnesses.
View Transcript
We've come a long, long way with the understanding that depression is an illness, that suicide as an outcome of depression or anxiety is a tragic outcome. I mean, if somebody dies of cancer, we just all see that as tragic. But a much smaller percentage of people see someone dying of suicide who had a depressive illness as the same tragic outcome, bad outcome of a medical disorder. It's sad, but it's as if they had just been stronger or something, you know? Weakness of character issue. Even though the data is just overwhelming that these are medical illnesses no different than diabetes and hypertension.
Levine asks if that’s what worries him. Jordan nods. He explains his financial challenges, from his low-paying grocery store job to his increasing health insurance premiums to his high heating bills during the winter. His filled prescriptions are still waiting to be picked up at the pharmacy because he can’t afford the co-payments.
“I can imagine why you’re worried,” Levine says. “I still think it’s important to arrange for the iron infusion, and then we will figure out the costs before you go, OK?”
Levine sits with Jordan while he calls the Infusion Center to schedule the treatment. Meanwhile, she emails the staff underscoring the urgent need for Jordan to be seen. This is how progress happens in the primary care clinic Levine runs at the Massachusetts Mental Health Center, which is operated by the state’s Department of Mental Health in partnership with the Brigham. The center provides comprehensive care for people in greater Boston who live with major depression, schizophrenia, bipolar disorder, and other serious mental illnesses. Levine’s clinic is designed to support patients like Jordan who have complex medical needs, as well as people experiencing homelessness, substance use disorders, and trauma.
This integration of primary care and mental health care is especially critical, she says, because 60% of the center’s patients die from reversible causes, including complications from diabetes, heart disease, smoking-related illnesses, and hepatitis.
“After years of working with my patients, the separation of their mental and physical health began to seem false,” says Levine. “I can provide much better care for them when their primary care and mental health care are integrated.”
XI. Leveraging primary care
Nationwide, primary care doctors like Levine are increasingly the preferred avenue for people to receive mental health services. General practitioners now prescribe 80% of all antidepressants, the most common type of medication prescribed in primary care. Evidence strongly supports this movement to receiving mental health care within primary care.
The IMPACT model shows that savvy social workers and health coaches can provide meaningful, important work you don’t need a face-to-face evaluation with a psychiatrist for.
Jane Erb, MD
In December 2002, the Journal of the American Medical Association published the results of a landmark research study called IMPACT: Improving Mood–Promoting Access to Collaborative Treatment. In the IMPACT model of care, a circle of providers—including social workers, care coordinators, specialist nurses, and consulting psychiatrists—collaborates with primary care physicians to offer patients personalized mental health services.
“More than 80 studies of the IMPACT model show patients had outcomes that were over twice as positive as patients who received mental health services in the usual way, such as a simple prescription and follow-up appointment or a therapy visit with an on-site mental health specialist,” says Jane Erb, MD, the Brigham’s lead psychiatrist for implementing the IMPACT model in primary care. “Repeated follow-up studies using the IMPACT model, at the Brigham and elsewhere, also show improvement in these patients’ general health, with lower overall healthcare costs.”
Members of the collaborative care team, including Jane Erb, MD (left), review patient cases at Advanced Primary Care Associates at South Huntington. (Photos by Stu Rosner)
In 2011, Advanced Primary Care Associates at South Huntington was the first Brigham practice to adopt the IMPACT care model, which all Brigham Health primary care locations use today.
One afternoon each week, Erb meets with South Huntington’s collaborative care team to discuss their cases. During one of these meetings, care coordinator Vilma Alvarez pulls up the chart of a middle-aged patient, Claudia*, and the team cheers. Claudia’s high depression scores have dropped over several sessions since she started meeting with Alvarez.
“Great work!” Erb says. “This shows a huge improvement in patient-provider trust. This patient has never before remained engaged in any treatment recommendations.”
The team members, who are all trained in health coaching, behavioral activation, and cognitive behavioral therapies, dive into Claudia’s case.
Sounding the alarm on burnout
Leaders at the Brigham are taking a significant stand against burnout, starting at home.
Hearing how well Alvarez connected with Claudia, the group brainstorms ideas, including free wellness classes and internet-based cognitive behavioral therapy. For two years, the Brigham’s primary care practices have guided patients through this evidence-based online course, which teaches about the cycle of depression and anxiety, how to challenge negative thoughts, and how to apply these ideas to their lives. The course is free and can be accessed from home without any waiting period, making it ideal for people who have busy schedules or skepticism about therapy.
“The IMPACT model shows that savvy social workers and health coaches can provide meaningful, important work you don’t need a face-to-face evaluation with a psychiatrist for,” says Erb. “These folks reach out proactively with phone calls, virtual visits, and prescribed check-in intervals to measure patients’ depression and anxiety. They also identify activities the patient can begin to participate in that will hasten improvement and prevent relapse.”
Erb adds, “This model enables us to magnify our impact by advising collaborative care teams who work with hundreds of patients in settings where they prefer to be seen.”
*All patient names have been changed to protect privacy.
4
Weathering
Multiple Illnesses
We are identifying opportunities to change a patient’s emotional trajectory so they walk away from a potentially traumatic experience with knowledge and growth.
XII. “There’s more to survival than physical recovery”
Improving access to mental health services requires meeting patients where they are, whether through a virtual visit, a primary care checkup, or even at their hospital bedside.
Many patients in the Intensive Care Unit (ICU) deal with twofold trauma: 1) the catastrophic injury or health crisis that brought them there and 2) the stresses of being hospitalized. They often drift in and out of consciousness, hooked up to a ventilator, while their bodies fight to stay alive.
These fragile patients often struggle with hallucinations or nightmares that seem as real as actual memories. Numerous studies show up to 80% of ICU survivors experience this kind of delirium, and an estimated 20% are later diagnosed with post-traumatic stress disorder (PTSD) related to their hospitalization.
Psychiatrist Nomi Levy-Carrick, MD, MPhil, meets with ICU patients to help them make sense of their traumatic experiences during and after their admission. Her work is part of a unique, proactive psychiatric consultation model that brings trauma-informed care to patients at some of their most medically vulnerable moments. During patients’ time in the ICU and their subsequent stays in other units, Levy-Carrick follows them to help stabilize their mental health.
As a psychiatric consultant to the Brigham’s Critical Illness Recovery Program, she also meets with patients after their discharge home. She says, “After the dust settles, we can fill some gaps in a patient’s memory and tether some of their confusing or terrifying hallucinations to actual experience.”
A frequent delirium-induced nightmare among ICU patients is imagining balloons and bobbing heads floating around their beds.
“To some people, it can be helpful to clarify that, ‘What you saw were all the nurses, anesthesiologists, pulmonologists, and respiratory therapists standing around your bedside, working together to optimize your care,’” she says. “People can find some comfort and start to process that experience without the emotional distress that was attached to it before.”
Brigham researchers found that, among patients with respiratory failure, proactive psychiatric consultation resulted in shorter hospital stays than with conventional care.
“There’s more to survival than physical recovery,” she adds. “We are identifying opportunities to change a patient’s emotional trajectory so they walk away from a potentially traumatic experience with knowledge and growth instead of functionally impairing symptoms, including PTSD.”
Another Brigham leader in trauma-informed care is Annie Lewis O’Connor, PhD, NP-BC, MPH, founder and director of the C.A.R.E. (Coordinated Approach to Resilience and Empowerment) Clinic. Started in 2011, the clinic assists victims of interpersonal violence such as domestic and sexual violence and human trafficking.
6key principles of a trauma-informed approach
Safety – everyone’s physical and psychological safety is a top priority
Trustworthiness and Transparency – all share a commitment to transparently building and maintaining trust among everyone in the organization
Peer Support – engaging peers to promote recovery and healing
Collaboration and Mutuality – everyone has a role to play in creating a healing, therapeutic environment
Empowerment, Voice, and Choice – shared decision-making empowers everyone
Cultural, Historical, and Gender Issues – respecting and responding to each individual’s racial, ethnic, and cultural needs
Abridged from SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. HHS Publication No. (SMA) 14-4884. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2014.
Listening to and strategizing with patients about their priorities is an essential aspect of trauma-informed care, Lewis O’Connor says. For example, she explains, if a woman comes to the ED with injuries from domestic violence and she also has high blood sugar levels, her top priority may be dealing with domestic violence or depression and how that is affecting her health. Her diabetes may be a much lower priority, which can put her at odds with her care team.
In recent years, Lewis O’Connor has been sharing her knowledge of trauma-informed care across Partners HealthCare, which includes Brigham Health. An instructor at Harvard Medical School, she teaches medical students to look at the traditional provider-patient relationship from a new perspective, understanding that most people have experienced some form of trauma in their lives.
“We need to change the hierarchy of ‘I’m the physician’ or ‘I’m the nurse practitioner, so I know better than you,’” Lewis O’Connor says. “We need to flip it to say, ‘While I have more knowledge than you about certain things, you are an expert in your life. Help us understand what you need and want.’”
XIII. “It’s such a relief to be able to give our patients options right away”
Like other serious illnesses, addiction weaves a tangled web of physical and emotional suffering. Multiple national surveys have found that 50% of people with substance use disorders contend with other mental health issues of the same sort as the general population. In regions hit hardest by the opioid crisis, that figure may be conservative.
In 2018, nearly 2,000 people in Massachusetts died from an opioid overdose, according to the National Institute on Drug Abuse. This rate is two times higher than the rest of the nation. And while the overdose death rate has been declining slowly in recent years, the number of overdose-related 911 calls continues to rise. Staff throughout the Brigham Health system have seen skyrocketing numbers of people with overdoses and injection-related infections or who are seeking addiction treatment.
Yet, as in virtually every other corner of the mental health care system, people with substance use disorders face long waits for inpatient and outpatient programs due to the scarcity of these services.
“When patients with addiction are sent right back to the community, they feel vulnerable, tend to use again, and this creates a vicious cycle,” says Tim Erickson, MD, an emergency physician and chief of the Division of Medical Toxicology.
At the beginning of the opioid crisis, the Division of Addiction Psychiatry launched a comprehensive outpatient substance treatment program on the Faulkner campus. The team worked to set patients up for successful recovery after discharge by initiating addiction treatment during their hospitalization.
“However, even when we discharged people with referrals to outpatient addiction treatment programs, 50% of them never made it to their first appointment,” says Joji Suzuki, MD, director of addiction psychiatry. “Even a two-week delay for follow-up appointments can be challenging for these patients. As a system, we needed to address this crisis in new ways and better coordinate different parts of the hospital already offering addiction treatment.”
The Bridge Clinic has cared for more than 400 patients to date, with a team of experts in addiction psychiatry, infectious disease, primary care, and more.
Christin Price, MD, describes the struggles faced by many people with substance use disorders that can interfere with access to treatment.
View Transcript
The retention rate that we have in care is really unique in the sense that, you're keeping people in care that have really not had any sort of longitudinal care, and actually, again, they are like not your average person who has a steady job or stable housing. So to have 70% of patients that are struggling with something that's really challenging, like Opioid use disorder and co-occurring mental health, and they often don't know where they're gonna get their next meal or housing. To keep them in care in six months, I think is, sort of really speaks to why a model like this works because a lot of times, just due to the nature of mental health illness and addiction, the kind of traditional healthcare setup, just isn't meant for patients that really have these chaotic lives. And there's still a lot of stigma out there, and I think that's another thing, is that they don't feel welcome in a lot of other programs or clinics. So, I think that's why it's like pretty significant that we have these great results for a patient population that itself, is already at such high risk.
Suzuki says this dilemma inspired the Brigham to create a program that initiates and continues addiction treatment immediately after leaving the hospital or emergency department. With philanthropic support, the Brigham Health Bridge to Recovery Clinic opened in the spring of 2018. Now, when these vulnerable patients are being discharged or leaving a primary care appointment at the Brigham, they can walk down the hall to the clinic.
“It’s such a relief to be able to give our patients options right away,” Erickson says. “Often, patients with addictions get stereotyped that they don’t want help. This could not be further from the truth. They do not enjoy being addicted and want a way out. They just need options and the means to do it.”
The Bridge Clinic was designed to provide treatment for weeks or months while patients are waiting for openings in longer-term addiction programs.
“Addiction is a chronic, treatable medical condition,” says Christin Price, MD, the clinic’s program administrative director. “We need to treat the changes in the brain caused by substances. The overall rates of recovery for substance use—when providing effective medications, support, and therapy—can often be better than outcomes for obesity and diabetes. The main issue is patients don’t often have access to timely treatment.”
Price adds, “When we address patients’ immediate needs first, such as prescribing medication for the addiction or helping them apply for housing and other social services, they can focus on unpacking the trauma in their lives.”
XIV. Remarkable transformations
When Jeff* first came to the Bridge Clinic eight months ago, he lived under a bridge, injected heroin and fentanyl, and suffered from severe anxiety and PTSD.
Nearly 70% of bridge clinic patients have stayed in treatment for 6 months or more.
“He was so anxious he would only see one provider here; he wouldn’t talk to anybody else,” Price says.
Since getting treatment, Jeff reconnected with his mother. Now, he is living with her, seeing a therapist, and no longer uses heroin and fentanyl. He also volunteers at a food pantry.
“With his anxiety, he wouldn’t have been able to sit in a room with other people, and now he’s actively volunteering,” Price says. “In a matter of months, the transformation has been remarkable. Yes, the addiction is what got him here, but addressing the PTSD and anxiety is what helped him recover.”
Jeff is one of more than 400 patients cared for so far at the Bridge Clinic by a small team including infectious disease experts, a primary care physician, addiction psychiatrists, a resource specialist, and recovery coaches who offer peer support. The clinic also works closely with a social worker specializing in trauma who offers ongoing therapy.
Confronting the mental health toll of cancer
Fremonta Meyer, MD, is a psychiatrist at the Brigham who specializes in helping cancer patients navigate anxiety, depression, pain, and other issues.
Appointments are not required. If a patient shows up and the provider is busy, another member of the team usually will see them. If a patient relapses with alcohol or drugs, the clinic continues to treat and support the patient on their path of recovery.
“Many other programs are unable to continue seeing patients when they relapse or continue to use intermittently,” Price explains. “We approach addiction like any other chronic condition: It is a lifelong process that involves a variety of treatments and lifestyle changes.”
While it opened with typical clinic hours from Monday through Friday, the clinic is expanding its hours to weeknights and weekends. Price and her team are also looking at new ways to guide patients through recovery, including art and music therapy.
Nearly 70% of patients who received care at the clinic have stayed in treatment for six months or more, whether at the Brigham or in their community. Among these patients, the hospital has seen close to a 50% decrease in the number of ED visits and hospital admissions.
“This success rate speaks to why a model like this works,” Price says. “When we understand recovery as a continual process that doesn’t happen overnight, and we compassionately treat patients’ underlying trauma and pain, the risk of relapse is lowered.”
*All patient names have been changed to protect privacy.
5
Arriving at Hope
Our approach to care is recovery-oriented. Part of this means getting to know patients and what their strengths are, not just seeing them as their individual diagnosis.
XV. “Every day gets better and better”
Trauma takes many forms. First, Kyle* lost his job after missing too many workdays for mental health treatments. Then, he learned he has a mass in his chest. Crushed by anxiety and depression, Kyle turned to alcohol, breaking six years of sobriety. When his alcohol use spiraled out of control, he was so worried about his safety, he took a cab to the Faulkner’s ED.
“The last two years have been a nightmare,” says Kyle.
After seven days of treatment in the hospital’s inpatient psychiatric unit, Kyle’s outlook is much different.
“When I first came here, I was a nervous wreck,” Kyle says. “But the people are great, from the mental health workers to nurses to kitchen staff to peer counselors. I’m getting a little anxious I’m leaving, but it’s apples and oranges compared to where I was days ago.”
Kyle braved many twists and turns leading to the Faulkner inpatient unit.
“I’m an average guy—I went to college, worked in IT [information technology], coached Little League for my kids,” he says. “All of a sudden there were days I couldn’t get out of bed. People would say, ‘What do you have to be depressed about?’ They don’t understand.”
After self-medicating with alcohol, he sought help 10 years ago through Faulkner’s Addiction Recovery Program.
“Back then, the staff talked about depression and anxiety, but I didn’t believe it,” Kyle says. “I thought I could stop drinking and everything would be normal. After finishing the program, I started my master’s degree and was doing stuff I never dreamed of before. I see now that even though the alcohol went away, the depression and the anxiety never did.”
Getting admitted to the inpatient psychiatric unit gave Kyle a chance to participate in intensive therapy, manage his medications, and learn new coping skills. Upon discharge, he will transition to the Partial Hospitalization Program.
“Just seven days ago, I got into a cab to go home and said, ‘You know what, take me to Faulkner Hospital instead,’” he recalls. “If I went home, Lord knows what would’ve happened. Instead, I came here and I feel like a million bucks right now. Every day gets better and better.”
XVI. New opportunities and emotions
More than 500 patients like Kyle come to Faulkner’s inpatient psychiatry unit each year in crisis. Upon arrival, the care team guides them through medical conditions, including depression, anxiety, mania, psychosis, and substance use.
“Our approach to care is recovery-oriented,” says Chris AhnAllen, MD, PhD, director of inpatient psychology. “Part of this means getting to know patients and what their strengths are, not just seeing them as their diagnosis. We involve patients in making decisions about their care.”
Since joining Faulkner in 2017, AhnAllen has introduced more evidence-based interventions, such as cognitive behavioral therapy. The unit also offers psychosocial group programming, including sessions on life skills, stress management, yoga, music, and peer support.
Judy Ashton, a former patient turned volunteer, leads a peer support group on the unit twice a week and meets with patients individually. Before Sunday morning meetings, Ashton brings newspapers and snacks and socializes with patients. Over the past decade, she has volunteered more than 4,000 hours of her time.
Judy Ashton (second from left) is a longtime volunteer and benefactor at the Faulkner. (Photo by Len Rubenstein)
Two additional certified peer specialists work part-time on the unit, connecting with patients one-on-one and facilitating peer group sessions. In addition to their work on the inpatient unit, these peer workers recently started a free Saturday group called Allies, for current and former Faulkner psychiatry patients looking for connection and encouragement.
If you’re out there and alone, seek help. There’s nothing better than support. You reach out to one more person, you cut your problem in half.
Kyle*, a patient of Brigham and Women’s Faulkner Hospital
“If you have psychiatric issues, you need somebody in your corner,” Ashton says. “Peer workers are uniquely qualified to do that because we can share from our experience. Learning skills that have worked for other peers gives people some agency over their illness. If they try some new tactics and develop new coping mechanisms, they can deal with hallucinations, paranoia, depression, or whatever symptoms they have.”
Ashton describes how peers’ perspectives can help navigate their illnesses.
“We help people recognize the symptoms that can lead them to be acutely ill, so they can learn skills or take actions to prevent catastrophe,” says Ashton. “Some people might notice they are becoming increasingly isolated, having trouble initiating social activity, feeling unusually irritable or anxious, or are eating more or less than usual. We ask them to pay attention to these symptoms and be honest with themselves that they may be nearing a crisis. Then, we brainstorm ways to counteract these symptoms and avert the crisis.”
John Fromson, MD, chief of psychiatry at Faulkner, says, “Patients rave about our peer support program. In addition to volunteering her time and knowledge, Judy’s philanthropy assists our psychosocial group programming, including peer support.”
Ashton and her family also funded construction of the Ashton Family Terrace, the inpatient unit’s secure outdoor space that provides patients with access to fresh air and opportunities to garden.
XVII. “We’re all entitled to hope”
Ashton observes it is common for people to feel it’s a life sentence if they or their loved one is diagnosed with a major mental illness.
“People can recover,” Ashton says. “I’ve seen it. I’ve done it. With the treatments we have available and not internalizing the stigma, people can do very well. They may need help at times, including different treatments or additional medicines. We give that to people with other illnesses, and we ought to provide that to the same extent to folks with behavioral health illness.”
She adds, “Sometimes in psychiatry and other medical fields, the focus is on what’s wrong. In my peer counseling, I make sure I focus on what’s right. What are the strengths that have gotten you this far? You’re not just a bundle of symptoms. You’re a human being who has struggled and who has a tremendous amount of courage. People need an enormous amount of courage to deal with these illnesses.”
Searching for Causes and New Treatments
Researchers at the Brigham are exploring cognition as a marker to improve treatment for mental illnesses.
Whether someone is dealing with a serious mental illness or stressful life event such as divorce, loss of a job, or any issue, Fromson encourages people to recognize when they may benefit from mental health care.
“People can tolerate a lot of psychic pain and debilitation before, or if ever, getting help,” he says.
Fromson’s metaphor for well-being is a three-legged stool whose legs are family, work, and community.
“If one of those legs gets pulled out because of a strain in your relationships, impaired ability to function at work, or something happens with your community or religious affiliation, it may be time to get help,” he says.
“We want to show people how to develop ways to deal with problems that will be helpful, not hurt them more.”
Thinking back on his own experience, Kyle says getting the support he needs has been life-changing.
“I want to tell others if you’re out there and alone, seek help,” Kyle says. “There’s nothing better than support. You reach out to one more person, you cut your problem in half. And you’d be amazed that people come out of the woodwork to help. If I didn’t ask for that help, things could be tragically different.”
Ashton echoes this feeling.
Judy Ashton recounts a memorable interaction with a patient of the Faulkner’s peer support program.
View Transcript
I had a patient once when I told her my diagnosis and she said, "Wait a minute. I have that diagnosis. Are you telling me that I could do what you're doing?" And I said, "Yes. Everybody remember that!" It's a real amazing experience for patients. You know, one of the diagnoses people have when they go there is mine and they're just like, "Oh my gosh, she's got the badge, she's got the key. I can do that myself." So my presence lends a sense of hope for them. And I think for me it just reinforces what I already felt through my treatment that I'm going to be okay as life goes on.
“I will never forget the compassion shown to me by the exceptional staff in the Faulkner’s inpatient and partial hospitalization programs,” she says. “They helped me feel less isolated and taught me new skills to cope with my symptoms.”
Volunteering as a peer counselor has also helped Ashton’s recovery.
“My work as a peer counselor is the gift that keeps on giving to me,” she says. “It reinforces what I learn in treatment: I am going to be OK. More importantly, my presence gives patients hope for themselves.”
At a recent group meeting, Ashton listened as others spoke of their efforts to counter feelings that they are different because they have a psychiatric illness.
“I hope we can get rid of the stigma around mental illness,” Ashton says. “We’re all entitled to treatment for whatever illnesses we have. We’re entitled to support, and we’re entitled to feel a sense of hope. We’re all entitled to hope.”
*All patient names have been changed to protect privacy.