Like many people, Karen navigated challenges in her pursuit of parenthood. Over 10 years, she and her husband endured 17 rounds of IVF (in vitro fertilization) and two miscarriages.
Finally, Karen’s dream of getting pregnant came true. “When I got pregnant the third time, everything was going great,” Karen says. “At 10 weeks, I went for my ultrasound, and the technician saw something they didn’t like. They recommended I get a 3D ultrasound.”
At 13 weeks, on Christmas Eve, Karen got the more advanced scan.
“The technician started the scan and almost immediately left the room,” Karen recalls. “Then a radiologist came in and asked if I’d had an accident recently. No. Have I fallen down? No. Been in a car wreck? No. Gotten hit or kicked in the stomach? No. With each question, my heart sank a little more. By the last one, I knew it was bad.”
Their longed-for baby was growing, except all its organs were outside its body.
“My husband and I had invested so much time, effort, and money in IVF to get this baby, but we didn’t want the baby to suffer,” she says. “To be forced to carry that baby to term would have been horrific for that poor baby and me.”
Like many people, Karen and her husband decided to end the pregnancy. Fortunately, Karen had been getting her IVF and prenatal care in Boston at Brigham and Women’s Hospital, making the long drive from their home in New Hampshire. Their ability to rely on the Brigham’s complete array of expert reproductive healthcare is rooted in decisions made more than 50 years ago.
A test of new leadership
In January 1973, Kenneth J. Ryan, MD, was named chief of staff of the Boston Hospital for Women, which later evolved into Brigham and Women’s Hospital. Ryan was a national leader in obstetrics and gynecology (OB-GYN), a renowned scientist and medical ethicist. He completed his residency years earlier at the Brigham’s oldest predecessor, the Boston Lying-In Hospital.
Three weeks after Ryan assumed his new leadership role in Boston, the U.S. Supreme Court issued the Roe v. Wade decision, legalizing abortion nationwide.
“The hospital public relations office called and insisted that I give an immediate press conference so they could deal with a barrage of calls from the news media,” Ryan recalled in his 1993 President’s Address to the 10th annual meeting of the American Gynecological and Obstetrical Society.
“At the conference, I welcomed the Supreme Court decision to make abortion largely a matter between a woman and her physician and hoped there would be enough medical support in Massachusetts so that patients would not have to travel for care,” Ryan said. “My short vignette on all the television channels was followed by Archbishop (later Cardinal) Humberto Medeiros of Boston asserting that abortion was nothing less than murder. It was a chilling reception to the new politics of abortion.”
Reproductive Justice
“The human right to maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities.”
As defined in 1997 by SisterSong. SisterSong is the largest national multi-ethnic reproductive justice collective.
Facing the controversy, Ryan told the Boston Globe on January 28, 1973, that the Boston Hospital for Women was planning for as much as a 100% increase in the number of abortions it performed, the only area teaching hospital planning such an expansion.
“The Supreme Court ruling allows us to provide optimal care by putting the abortion issue where many felt it belonged in the first place—with the patient and her physician,” Ryan said.
Before the year ended, Ryan established an outpatient abortion service and an abortion and family planning training rotation for OB-GYN residents. Both programs were firsts at U.S. academic medical centers and have run uninterrupted for 50 years, outlasting Roe itself.
In Ryan’s footsteps
Robert Barbieri, MD, completed his OB-GYN residency under Ryan’s leadership in the late 1970s and early 1980s.
“Dr. Ryan had a great gyroscope for what was right,” says Barbieri. “He was a fierce advocate for his patients, and deeply committed to the ethics of keeping medical decisions between patients and their doctors.”
In 1993, Barbieri succeeded Ryan as chair of the Department of Obstetrics and Gynecology. One legacy of Barbieri’s leadership was establishing the Division of Family Planning as an official subspecialty within the department, on equal footing with other divisions.
Barbieri’s successor, Nawal Nour, MD, MPH, did her first rotation at the Brigham as a Harvard Medical School student just after Ryan retired. Later, she completed her residency at the Brigham.
I’ve spent my whole professional life at the Brigham, largely because of our longstanding commitment to equitable access, attention, and treatment for everyone who needs our care.
Nawal Nour, MD, MPH
“I’ve spent my whole professional life at the Brigham, largely because of our longstanding commitment to equitable access, attention, and treatment for everyone who needs our care,” says Nour. “I’m proud of our history as a national, even global, leader in providing the full range of reproductive healthcare services to everyone who needs them.”
Another voice of experience
“I started my residency at the Brigham in 1976, three years after Roe,” says Laurent Delli-Bovi, MD, a longtime Brigham OB-GYN. “I was lucky to train with Dr. Ryan and his colleagues, who were paragons of providing safe abortion care because they had seen so many horrible consequences of unsafe abortions.”
After residency, Delli-Bovi was medical director of five different family planning facilities, including the Brigham’s Division of Family Planning.
Delli-Bovi recalls, “One case I’ll never forget was a 32-year-old woman, mother of two small children, 23 weeks pregnant, newly diagnosed with advanced lung cancer. She and her husband didn’t want to continue the pregnancy and risk leaving him with two kids and a premature infant.
“Our patient was so sick, we had to perform the abortion in the main operating room,” Delli-Bovi says. “I remember someone in the room asked, ‘But why did she wait so long to end the pregnancy?’ I was stunned by what seemed like a lack of empathy. I finally blurted, ‘She just got diagnosed with late-stage lung cancer!’”
In 1992, Delli-Bovi co-founded Women’s Health Services, an independent clinic providing safe, skilled, compassionate care to all seeking abortion and family planning services.
“I became an OB-GYN to provide all the care women need,” says Delli-Bovi. “For me, abortion is not a question of choice; it’s a question of health and healthcare. Not all women, pregnancies, or fetuses are equally healthy. Not all pregnant people are dealing with the same economic, mental, and physical health issues. I believe bodily autonomy is a fundamental human right. Forcing everyone who gets pregnant to give birth is autocratic.”
Did You Know
Over the past 50 years, there have been at least 11 murders, 42 bombings, 196 arsons, and 491 assaults against abortion providers in the United States.
An unshakable commitment to care
This fierce commitment to patients is common among abortion and family planning practitioners.
“I feel so strongly about the need for abortion because patients need the care,” says Alisa Goldberg, MD, MPH. “When I was a resident at the Brigham, I saw how grateful the patients are. Seeing women taking control of the future they wanted and being able to help them do that was, and is, profound.”
After finishing her residency in 1998, Goldberg was among the first 10 OB-GYNs to complete the Family Planning Fellowship at the University of California, San Francisco (UCSF). The fellowship was created in 1992 by Philip Darney, MD, MSc, another trainee of Ryan’s. The fellowship provides two years of advanced training in clinical care, research, and health policy in abortion and contraception.
“By the 1990s, Dr. Ryan and many others who saw firsthand the deadly consequences of illegal abortion—and the dramatic decline of maternal mortality that followed Roe—were in their 60s and about to retire,” says Goldberg. “It was called ‘the graying of abortion providers.’ Amid the surge of anti-abortion violence in the 1990s, there weren’t a lot of people around willing, or able, to replace them.”
Goldberg continues, “Back then, the Family Planning Fellowship was more of an informal apprenticeship at UCSF. Over the past 30 years, it’s become a nationwide program and a formally recognized subspecialty of OB-GYN, tasked with expanding the field of experts in complex family planning and growing the next generation of leaders.“
Part of this generation herself, Goldberg returned to the Brigham in 2003 to establish the fellowship program, which she still directs. The Brigham is one of 29 academic medical centers around the country offering the Complex Family Planning Fellowship.
Building a sustainable future for reproductive healthcare
The breadth and promise of the fellowship were muted by a lack of OB-GYN residents being formally trained in abortion and contraception.
Seeing women taking control of the future they wanted and being able to help them do that was, and is, profound.
Alisa Goldberg, MD, MPH
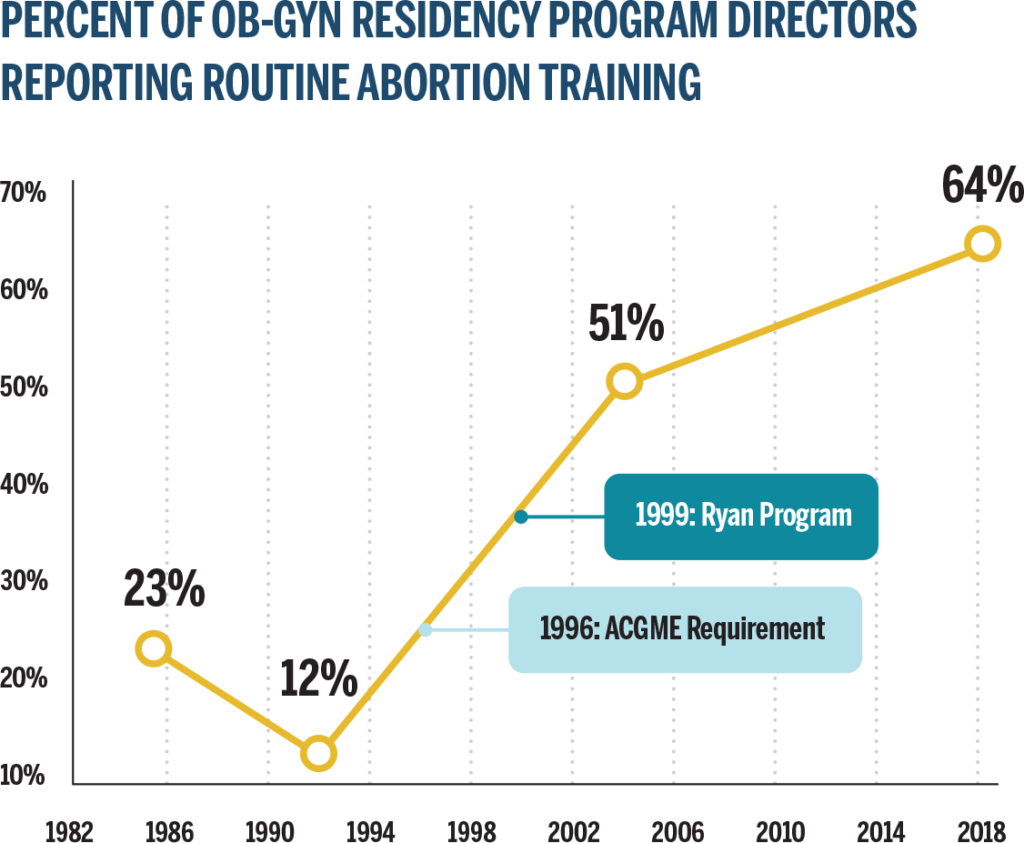
“In the years after Roe, many hospitals stopped providing abortion services, ceding the work to growing numbers of feminist community health centers,” says Goldberg. “Community-based centers provided great care, but residents and medical students largely weren’t going there to get training. So a whole generation of clinicians came out of medical school and residency without training in contraception and abortion.” (See figure below.)
In 1996, the Accreditation Council for Graduate Medical Education responded to this gap by mandating that OB-GYN residents complete a rotation in abortion and contraception. To ensure OB-GYN residencies adopted a uniform and robust curriculum to meet the requirement, the Kenneth J. Ryan Residency Training Program in Abortion and Family Planning was created in 1999. A living tribute to Ryan’s profound legacy in the field, the Ryan program was founded by Uta Landy, PhD, a leading abortion and family planning counselor, researcher, writer, and advocate.
The Ryan Program works with OB-GYN residency programs nationwide to integrate formal training in abortion and contraception for OB-GYN residents. Ryan Programs have trained more than 7,000 residents in abortion and family planning since their inception. As of 2022, there were 109 Ryan Programs in the U.S. and Puerto Rico.
Source: The Kenneth J. Ryan Residency Training Program in Abortion & Family Planning website
“Not every OB-GYN residency includes a Ryan Program,” Goldberg explains. “Where it does, you know those residents are getting rigorous training and education in every aspect of abortion and family planning care.”
However, future training in abortion and family planning for OB-GYN residents is at risk in the wake of the Supreme Court’s ruling in Dobbs v. Jackson Women’s Health Organization. Currently, Dobbs leaves more than 70% of U.S. medical students training in states with restrictive abortion laws or outright bans. Only 29% of the more than 129,000 medical students in the U.S. will train in protected states. That number could continue to shrink as more states enact abortion bans or restrictions.
Changing outlook
Another challenge in training a new generation of abortion and family planning leaders stems from moral or religious objections to abortion among residents. When the training is mandated, the requirement includes an opt-out clause for residents with moral or religious objections to abortion.
When Pat Doe1, MD, began the OB-GYN residency at the Brigham, the young doctor planned to go through the family planning rotation as a partial participant, opting out of abortion care.
“I’m from a close, religious family with strict views against abortion,” Doe says. “I started just observing in the abortion clinic. But as I saw the infinite variety of circumstances of the people coming to us for abortions, I realized how essential abortion care is to my training as an OB-GYN, so I started participating.” One unforgettable day also helped change Doe’s outlook.
Did You Know?
If all abortions in the United States were to stop:
24%
more people would die from pregnancy complications and
39%
more non-Hispanic Black people would die.2
“At one point in the residency, I spent the morning in the family planning clinic and the afternoon on labor and delivery,” Doe recalls. “In the clinic, I’d done a second-trimester D&E [dilation and evacuation abortion procedure]. Later that day, I walked across the hall to labor and delivery, where a patient’s membranes had ruptured at 20 weeks. That woman needed the same procedure, a D&E, as my morning patient. It was a clarifying moment of understanding abortion as basic healthcare. It’s been humbling to question the ethics I was raised with.”
Doe’s initial view of abortion as an irresponsible choice has shifted through working with the wide range of patients in the family planning clinic.
“Now, I can see abortion as a profound expression of respect for parenthood,” Doe says. “I had a patient, six weeks pregnant, using multiple substances, including cocaine and heroin, in an unsafe relationship, housing insecure—an unimaginably difficult situation. She came to us wanting an immediate termination, but there were various barriers to her abortion care, including active substance use.”
Doe continues, “We spent eight weeks getting a safe plan of accompaniment organized for her pregnancy termination. Clearly, this patient had enough respect for the responsibilities of parenthood to know she could not become a parent at this time in her life. It was a beautiful experience to support her in that decision.”
Battling misinformation
While education in abortion and family planning is integral to quality reproductive care, it also helps counter the misinformation and disinformation that fuel abortion bans and restrictions.
“Everybody, including medical professionals, is fed so much misinformation and disinformation about abortion,” says Deb Bartz, MD, MPH, director of the Brigham’s Ryan Program. “I have a strong desire to counter that with realities of what abortion care is, who our patients are, and what the abortion workforce looks like.”
She adds, “My mission is working with medical students and residents to inspire them to become abortion providers themselves or to at least be able to provide high-quality referrals. It’s also important that any physician, and especially an OB-GYN, be able to talk intelligently and factually about abortion when they sit on medical committees and in institutional leadership roles.”
Abortion is not an easy decision, but it’s so important to be able to make it when you need to, without anyone judging or shaming you for doing it.
Karen, patient
Bartz believes the Dobbs decision is due, in part, to a lack of leadership by the medical establishment to combat the stigma associated with abortion.
“It’s on all of our shoulders that Roe fell,” she says. “Abortion care was relegated to the community in so many cases, and much of academic medicine was fine with that. We need to be very reflective about the medical community’s contribution to the Dobbs decision.”
Still, Bartz is hopeful that the Ryan Programs in places that restrict or ban abortions will be able to reach students and residents in those states.
“Most states with a medical school have at least one institution with a Ryan Program,” she says. “It’s a rigorous program with strict requirements for educational quality and presence of expertise. We have high-quality family planning specialists everywhere working hard to get the training across to residents and students in states with bans or restrictions.”
Who Gets Abortions?
1 in 4
women will have an abortion by age 45
61%
already have children
75%
are low income or poor, with limited or no access to health insurance
62%
are religiously affiliated
55%
have had a disruptive life event, such as death of a family member or close friend, job loss, termination of a relationship with a partner, or overdue rent or mortgage obligations
Care Centered in Compassion
When Karen and her husband came to the Brigham for the abortion, they were relieved by the support they received.
“It was such a warm and caring environment,” she says. “Everyone was fantastic, and I have such high regard for them. Luckily, these doctors, nurses, and counselors can help us make these difficult decisions. Abortion is not an easy decision, but it’s so important to be able to make it when you need to, without anyone judging or shaming you for doing it. I wish people were more open-minded and could discuss this without so much judgment and shame.”
Central to the Ryan Program curriculum is a values clarification process to help residents identify and overcome biases that lead many people to view abortions on a spectrum of good to bad. Likewise, ensuring each patient feels cared for and supported is vital to the mission of the Family Planning Center.
“People are so surprised to get such good treatment here,” says Colleen, a Brigham nurse in the center. “We know how scared and vulnerable our patients can feel when they come here: for their physical safety, for being judged. We’re all trained to treat and talk with people without judgment. Because there’s no one kind of person who gets an abortion. It’s everyone.”
Colleen adds, “Our patients always leave better than when they came in, which gives so much meaning to my life. This is the greatest place to work because our mission feels like a calling. I don’t want to do any other kind of work.”
Liz Janiak, ScD, MSc, MA, is a public health researcher and educator at the Brigham and Harvard University. She has seen firsthand how abortion stigma can make people feel their own abortion is unique and essential but withhold empathy for anyone else.
“The biggest surprise of my career is how abortion stigma gets internalized and comes out as judgment toward other people in the same circumstances,” Janiak says. “It still stuns me how many patients think the only ‘good’ abortions are for rape, incest, and whatever they have going on in their own lives.”
Striving for reproductive justice
As a researcher and educator, Janiak believes academic medicine has a vital role in eliminating abortion stigma: for patients, providers, and in the broader public discourse.
“We are the top OB-GYN department in the country,” says Janiak. “And the Brigham and MGH [Massachusetts General Hospital] have a top OB-GYN residency in the country. There’s great power in telling the world that an essential part of being the best in the world at providing and training people in reproductive medicine is providing abortion and family planning services. I would love to see our commitment to supporting patient autonomy celebrated and elevated more, along with providing even more low- and no-cost care.”
Bartz adds, “Ken Ryan was a big, almost mythological hero to us. In the moment after Roe, he knew what was right, and he did it. That’s what we’re part of. And I think the Brigham’s example has bolstered other health systems to consider ways to be brave. The Ryan Program helps highly influential medical centers put abortion within their OB-GYN departments. Of course, family planning is part of our obstetric service. Of course, our patients need family planning.”
As an OB-GYN leader, Nour acknowledges that while Massachusetts has a generous legal system for abortion patients, there are more barriers to address.
“The Dobbs decision goes against reproductive justice, which has been our mission and inspiration going back to our previous department chairs, Ken Ryan and Bob Barbieri,” she says. “But we know from the Roe years that having a right and having access to exercise that right are two different things. Whether our patients desire pregnancies but their insurance doesn’t cover IVF or inseminations, or they have complex health issues and need contraception or want to figure out how to continue their pregnancies, or they need to end their pregnancies, we will continue to work on equity and access for all people, everywhere. It’s who we’ve been for 50 years and who we still are.”
1. Name changed upon request 2. Stevenson, Amanda J., et al. “The Maternal Mortality Consequences of Losing Abortion Access.” SocArXiv, 29 June 2022. Web.