
Geography has always dictated the standards of care available to physicians and their pregnant patients. The Dobbs decision has deepened this divide. Physicians treating a pregnant person in any of the 24 states (as of July 1, 2023) that ban or restrict abortion have vastly different care options available to them than if they were practicing in Massachusetts or one of the other 23 states where the right to an abortion is still protected.
This doesn’t only affect residents of states where abortion is banned. If a pregnant person visits one of the states that criminalize abortion and experiences a health emergency, their care will be dictated by the laws of that state, not the evidence-based standard of care available elsewhere. (See Maternal and Infant Mortality in the U.S. graphics below.)
A March 2023 lawsuit filed against the state of Texas by five pregnant women and two physicians documents the confusing, even life-threatening effects abortion bans have on physicians’ clinical decision-making:
“If a pregnant patient is experiencing renal failure, does she have to be on dialysis before a physician may perform an abortion that would otherwise be prohibited by the Ban? If a pregnant patient has a cardiac lesion, does a physician have to wait until she experiences heart failure to intervene? If a pregnant patient has a clogged blood vessel, does a physician have to wait until she experiences chest pain before terminating the pregnancy to prevent pulmonary embolism?”
Another physician queried: “[I]f I and another physician judge that a woman’s neurological condition is so complicated by pregnancy that she might lose entirely the ability to breathe, and I perform a procedure, could another physician look at the patient’s chart after the fact and think that we overestimated the danger, or that we should have delayed the abortion to see whether the patient’s condition deteriorated?”
MATERNAL AND INFANT MORTALITY IN THE U.S.
Maternal and infant mortality rates are higher in states that ban or restrict abortion. Black adults and infants are most adversely affected by abortion restrictions. Additionally, a study of maternal mortality in the U.S. from 2017–2019 found that 84% of pregnancy-related deaths were preventable.3
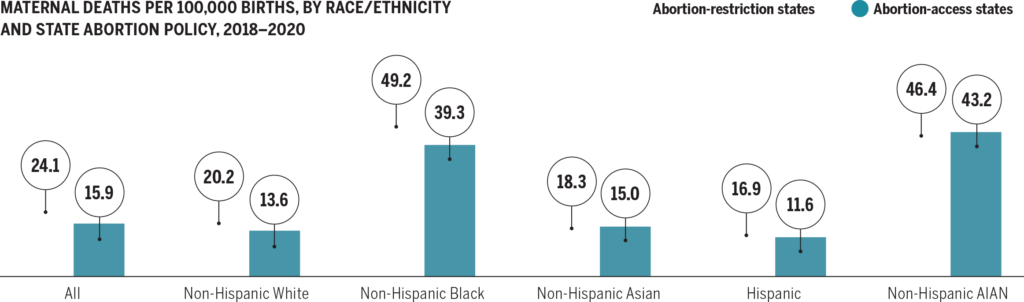
Note: AIAN = American Indian or Alaska Native
Data: Centers for Disease Control and Prevention, “National Center for Health Statistics Mortality Data on CDC WONDER,” last updated Dec. 22, 2021.
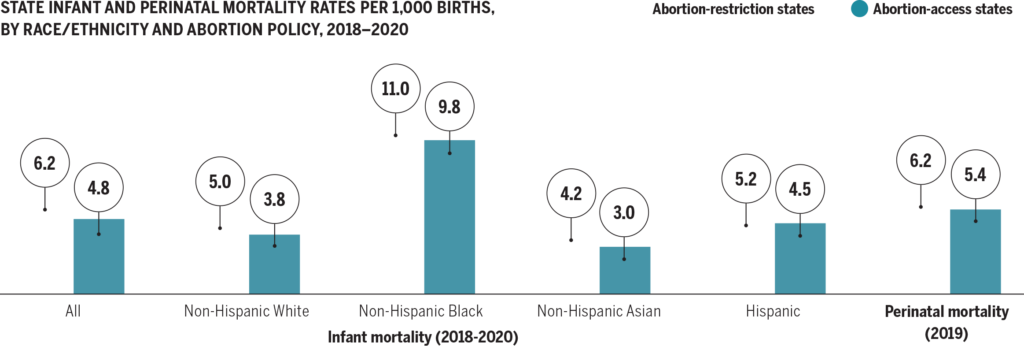
Data: Mortality — Centers for Disease Control and Prevention, CDC WONDER (database), “Underlying Cause of Death, 1999–2020,” accessed Sept. 30,2022; Perinatal mortality — Claudia P. Valenzuela, Elizabeth C.W. Gregory, and Joyce A. Martin, Decline in Perinatal Mortality in the United States, 2017–2019, NCHS Data Brief no. 429 (National Center for Health Statistics, Jan. 2022).
Source: Eugene Declercq et al., The U.S. Maternal Health Divide: The Limited Maternal Health Services and Worse Outcomes of States Proposing New Abortion Restrictions (Commonwealth Fund, Dec. 2022). https://doi.orh/10.26099/z7dz-8211
3. Trost SL, Beauregard J, Njie F, et al. Pregnancy-Related Deaths: Data from Maternal Mortality Review Committees in 36 US States, 2017–2019. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2022.